In Franz Kafka’s The Metamorphosis, Gregor wakes up to find that his “anxious dreams” are in fact reality: he has been changed into a “monstrous verminous bug” (1). Late for work, he struggles to free himself from the confines of his bed but is unable to escape. His family begins to knock anxiously on his door, and his manager scolds him angrily for his tardiness. Gregor tries to respond in self-defense, but he can no longer speak in words and is not understood by the others. With great effort, Gregor makes his way to the door; at the sight of Gregor, the manager departs hurriedly and the family stands aghast.
Gregor’s ill state has been established, and he is kept in his room. His sister feeds him and takes care of him eagerly at first, keeping his room clear so he can crawl around. His father seems to stay strong in denial while his sensitive mother pines. Gregor hides from his family by situating himself under the couch and shielded by a sheet. On one occasion, Gregor’s mother faints at the sight of her son and Gregor’s father lashes out at him, throwing apples that result in an immobile state of injury for Gregor.
Since Gregor had been the primary breadwinner for the family, each family member is forced to step up and take on new responsibilities for pay. The family takes on three tenants to help pay for rent. When they see Gregor, they immediately decide against the lease, disgusted by the familr. For the Samsa family, this is the last straw. Gregor is no longer a “he” but an “it” instead, which allows them to forfeit their claim and responsibility for him. That night, Gregor dies. Gregor’s death frees the Samsa’s, for their lives no longer need revolve around him, and they are able to return to a state of normalcy.
I have always found Kafka’s works to be incredibly compelling, and this one certainly did not disappoint me. One of the things that I found to be most fascinating was the role of the 3rd person omniscient narrator. Although the story seemed to be told through the eyes of Gregor, the narrator was not inside his head but rather an objective observer. I felt that the narrator’s intimacy with Gregor was transformed just as Gregor’s own transformation evolved throughout the novella. As Gregor’s insect identity became more and more consuming, the narrator joined the Samsa family in distancing himself from Gregor. If anything, this shows just how isolating Gregor’s insectification really was- even the narrator who is telling his story abandons him.
—
Discussion Questions:
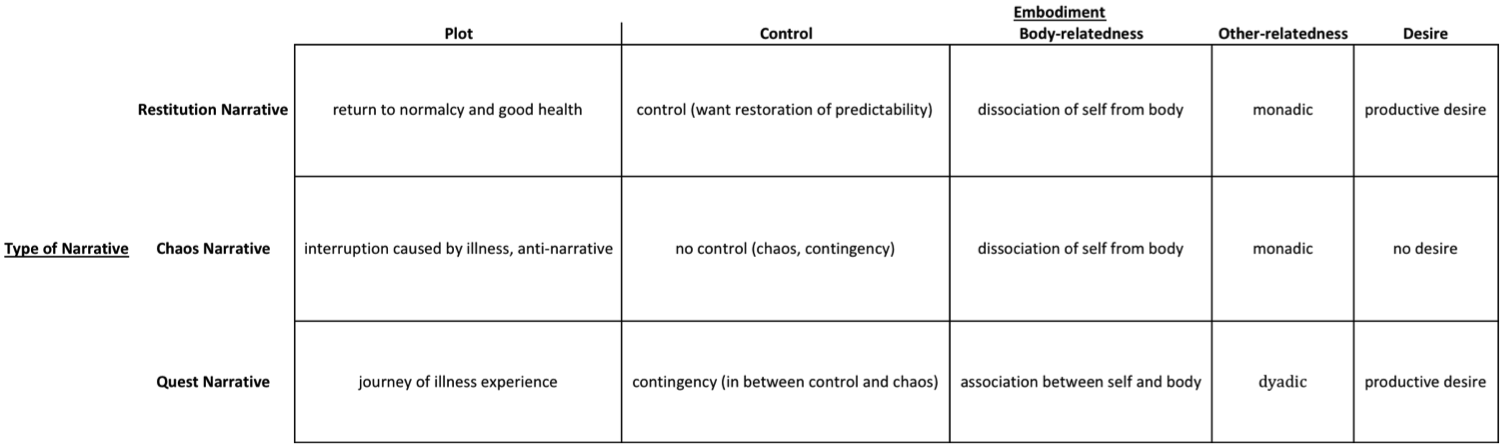
1. What parts of the text can be identified as representative of a chaos narrative? A quest narrative? A restitution narrative?
2. What words does Kafka use to allude to Gregor’s insect-like state?
3. What is the effect of the 3rd person narrator? How does the narrator’s stance evolve throughout the novella?