Standing before us were four individuals: a public health professor, a director, an actor, an artist. But each of these individuals held so much more than just one profession; they each dabbled into a variety of other realms, but they were all here for one reason. Today, they were here to promote the power of narrative.
Tell Me A Story: Designing Narratives for Health Behavior Change was an extraordinarily compelling and fascinating symposium organized by the School of Public Health.

With three prominent guest speakers each contributing their insight about a different facet of the narrative, this symposium explored essence of the narrative and the potential potency of its role in instigating change.
To begin with, Monte Montgomery showed the audience what makes a story. 4 purposes, often accomplished by a 3 act structure. Engaging, understandable, and memorable all lead to the fourth purpose: actionable. The 3 act structure, as illustrated below.

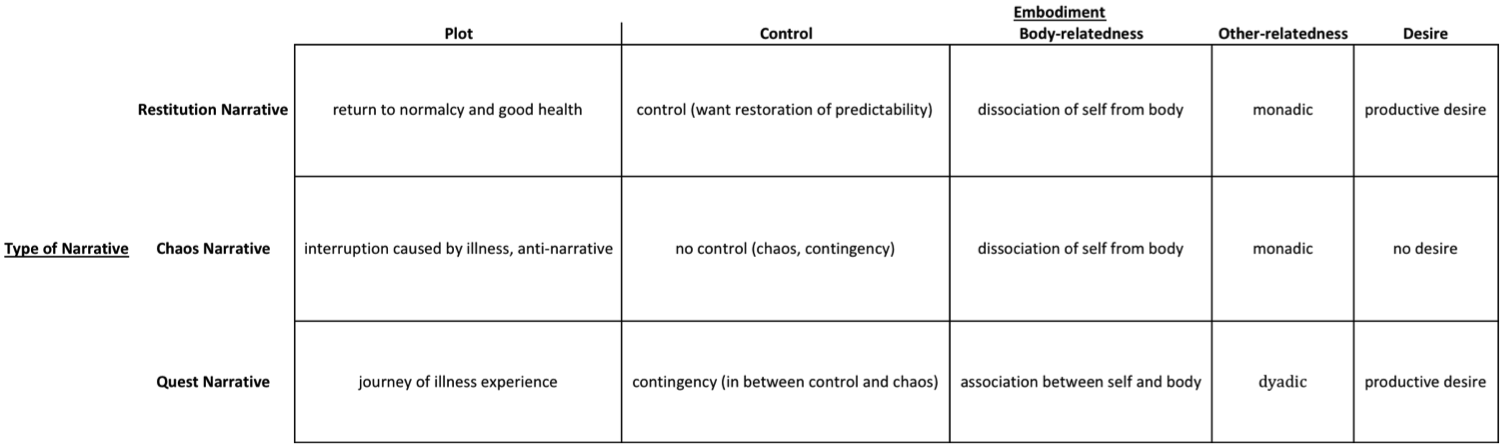
Although this 3 act structure seems to be relatively pervasive in our society, I found it interesting that illness narratives represent one of the few genres that often defy this standard. Just as disease pushes against the normal functioning of the body, illness is defined by a deviation from the norm. And since illness narratives are created to mirror the illness experience, illness narratives resists the 3 act structure.
So what are the effects of this resistance? The most powerful deviation in my mind was that while 3 act narratives imply that conflict allows for an individual to achieve greater stability. This in many ways embodies the triumph narrative, which Conway so persistently cautioned us about. The 3 act structure suggests that the restitution narrative allows for not only a restoration but a progression, where an individual becomes better off than they were in the past. Illness narratives that break free from the model of the triumphant overcome of illness, then, also escape the confinement of the 3 act structure.
After Montgomery had established a basic understanding of narrative and explored the individual change that narratives can inspire, Mike Mosallam discussed the social changes that can arise from narratives. Leading with the powerful question “What is my story?,” Mosallam gave us a glimpse of his own narrative and introduced us to his reality TV show All American Muslim to show how theater can instigate social change by creating dialogue, building bridges, and humanizing groups of people such as Arabs/Muslims.
One story that particularly struck me was Mosallam’s anecdote about acting as a patient for medical school students. Mosallam described how a key part of using narrative revolves around preserving the “authenticity of stories.” There were some medical students who he said he would never want to have as his doctor. “You can’t guide and manipulate,” he explained. “Let the subject direct the narrative.”
Taking a step away from the commonly linguistic nature of narrative, Kody Chamberlain walked us through the process and the power of incorporating art into narrative. He opened my mind to thinking more about what is entailed by the creative process, which is really an interdisciplinary challenge that shares many similarities between different realms. It was fascinating to think about the impact of images, especially in the spaces between words or as replacements to words. Chamberlain’s advice about the creative process, the persistence and the depth involved in works of art, was extremely interesting, and I felt like he dispelled many common stereotypes of art with ideas such as “inspiration is a placebo.”
These three speakers left us all with a challenge:
What do you want to do? How do you want to do it?
And how can you incorporate the power of narrative?